| Pages:
1
..
4
5
6
7
8 |
Zombie
Forum Hillbilly

Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
It's all good.
The more I begin to understand the more shocked I am at how little is actually completely understood.
Truthfully it is almost appalling that a Dr. will assign a diagnoses, prescribe a medication, and not fully understand what is happening. Worse yet is
the fact he may not understand the diagnosis.
Trained rats pull the correct lever.
I'm not starting a Dr. slam rant. Not at all. Im just surprised at how much some of you know in these discussions, and you are the first to say that
much of it is still unknown.
How much more can there be? Thousands of multi-syllable words, and they don't begin to cover everything... Surprising!
[Edited on 4-26-2015 by Zombie]
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
cyanureeves
National Hazard
Posts: 744
Registered: 29-8-2010
Location: Mars
Member Is Offline
Mood: No Mood
|
|
i hope they do one day find a good anti depressant that works for all the world and completely different than todays popular medicines.i mean one time
i took a blotter that was just so wonderful and felt so peaceful and happy that i was the happiest day of my life.granted everything around me looked
magenta colored but it was an acid so different.this 2015 by golly and marihuana is legal in some states because alot people just had enough of what
they believe were lies.if not for the whole world then at least to the severe manic because they will be better than the walking dead crap they get
today.i would like to see the elderly in a happy mood even if it's in a magenta world.i so hate to see old folk fed crap that keeps them sedated all
the time and the elderly make up a huge part of anti depressant market.i am getting up in years and i just want to feel good but i really dont like to
be high, well i do but i dont also.we just need a good med.
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
I wouldn't be too quick to levy judgment against most physicians, even though the vast majority are not drug specialists. Physicians simply don't have
enough time to devote to being both a scientist and a clinician, nor do most of them have the training, in the vast majority of cases. An honest
physician (or nurse, or whoever) will admit this, even if they dislike it. To keep up with just the clinical journals is basically impossible, even if
that were the sole duty of a physician: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC521514/
Really deep analysis would take longer. If a physician lacks graduate scientific training, or desires to perform clinical work in addition to any
research, they have a greater problem than someone with a non-truncated PhD, bachelors', and no patients to see.
However, their physician differential diagnosis skills and generalized medical knowledge are unparalleled. They may not know a diagnosis with
certainty, or understand the etiology of a correct diagnosis, but they will likely understand it far better than anyone else, barring another
physician. What alternative is there? A PhD pharmacologist or a pharmacist may have a much better understanding of medications, specific formulations,
interchangeability, etc. but their ability to correctly differentially diagnose without very special training (partnered practices in a few states,
some VA hospitals, certain applied pharmacology fellowships, etc.) are limited because their background in pathophysiology is different. They may be
good for 9/10 ddx, but just as a typical physician without a specialization in pharmacology is unlikely to really know their non-prototypical drugs
offhand, it is rare for all but the most experienced PAs to really compare to the differential diagnosing training of a physician, and parse when a
mistake has been made as well as how best to try to resolve an issue.
The same could be said for surgical intervention... as some dental and pharmacy schools share gross anatomy cadaver labs with MD/DO students, yet are
clearly not as qualified as any medical student to deliver a baby or perform an appendectomy. I might consider a microbiologist as having far more
knowledge of P. aeruginosa than my general practitioner, and I am sure both could diagnose it adequately from culture (or their technicians could,
with a kit and some form of Bergey's Manual), but I would prefer the physician treat such an infection every time, just in case there were a
complication. Healthcare really is an interdisciplinary field, even just among physician specialties. If I need a heart surgery but have liver or
kidney complications, I may need a gastroenterologist or nephrologist to talk to my cardiologist. During the surgery, I need an anesthetist on hand. I
really don't see any viable alternatives given our knowledgebase keeps expanding, and so greater amounts of specialization are necessary. The problem
is even more difficult with psychological problems, with the implausibility of having labwork give you a definitive diagnosis, as definitive as a
diagnosis can be. Once psychiatry gets involved, you then have to discuss the psychiatry/psychology divide, which I am not qualified to speak on.
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
No judgement meant at all. Merely an observation of where medicine is. Everything you just posted was in my head I just use less words.
I'm sorry for distracting the thread. It needed some breathing room for us lessor educated to be able to follow the bouncing ball. 
Quote: Originally posted by cyanureeves  | | i hope they do one day find a good anti depressant that works for all the world and completely different than todays popular medicines.i mean one time
i took a blotter that was just so wonderful and felt so peaceful and happy that i was the happiest day of my life.granted everything around me looked
magenta colored but it was an acid so different.this 2015 by golly and marihuana is legal in some states because alot people just had enough of what
they believe were lies.if not for the whole world then at least to the severe manic because they will be better than the walking dead crap they get
today.i would like to see the elderly in a happy mood even if it's in a magenta world.i so hate to see old folk fed crap that keeps them sedated all
the time and the elderly make up a huge part of anti depressant market.i am getting up in years and i just want to feel good but i really dont like to
be high, well i do but i dont also.we just need a good med. |
I'm with you 100%.
[Edited on 4-26-2015 by Zombie]
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Nicodem
Super Moderator
Posts: 4230
Registered: 28-12-2004
Member Is Offline
Mood: No Mood
|
|
Back to depression... For those who like big data multivariate analysis, here is a very recent article using the data from the National Survey on
Drug Use and Health (2008-2012) (USA population):
Classic psychedelic use is associated with reduced psychological distress and suicidality in the United States adult population
J. Psychopharmacol., 2015, 29, 280-288.
DOI: 10.1177/0269881114565653
quote:
| Quote: |
...
We also cannot rule out the possibility that classic psychedelic
use may have caused harm at the individual level. Indeed, classic
psychedelic use may exacerbate schizophrenia or other psychotic
disorders, can be dangerous in hazardous physical environments,
and can sometimes elicit feelings of anxiety, fear, panic, and par-
anoia (Johnson et al., 2008). Nevertheless, the associations
reported here suggest that if individual-level harms occurred,
they failed to obscure the apparent protective effect of classic
psychedelic use on psychological distress and suicidality at the
population level. Considering that carefully controlled conditions
are ideal in the administration of classic psychedelics (Johnson
et al., 2008), it is noteworthy that naturalistic classic psychedelic
use demonstrated evidence of benefit. Not only could classic psy-
chedelic users have used in suboptimal settings, they could have
ingested substances of unknown purity and/or at sub- or suprath-
erapeutic doses. If the results do reflect salubrious effects of clas-
sic psychedelic use, these may very well be potentiated in
specialized treatment settings designed to maximize safety and
efficacy (Johnson et al., 2008).
...
Conclusion
Classic psychedelics carry a contentious recent history and
barriers to their clinical evaluation remain. Growing evidence
including the present research suggests that classic psyche-
delics may have the potential to alleviate human suffering
associated with mental illness. Further rigorous research is
warranted to better understand these substances, with the ulti-
mate goal of taking full advantage of their latent therapeutic
capacity. |
(The emphasis is mine.)
Efficiency under uncontrolled conditions surprises me as well.

[Edited on 26/4/2015 by Nicodem]
…there is a human touch of the cultist “believer” in every theorist that he must struggle against as being
unworthy of the scientist. Some of the greatest men of science have publicly repudiated a theory which earlier they hotly defended. In this lies their
scientific temper, not in the scientific defense of the theory. - Weston La Barre (Ghost Dance, 1972)
Read the The ScienceMadness Guidelines!
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
I actually meant to say anesthesiologist above, not anesthetist as the latter are nurses (not making a value statement).
Nicodem good find. Brand new!
That is a pretty big overall n, which I like, particularly to help support the study type. If the Araujo ayahuasca RCT placebo study finishes this
year as expected, I think it would be really interesting to see if any kind of comparisons can be drawn between reports from lifetime users versus
non-lifetime users just to see if any tentative generalizations could be drawn as to optimal presumptive treatment durations for investigation. Based
on the high comorbidity of anxiety disorders and depression as well as the common use of antidepressants in treatment, and the legend phrasing in the
first figure you graciously attached, it appears to me as though some of these studies, if properly designed, may also be used in support
of/conjunction with ongoing research into psychedelic anxiety disorder treatment. With an optimal target treatment duration derived from future data,
a comparison could be made with protocols such as recommended benzodiazepine treatment durations, the use of which may be contraindicated in depressed
patients (PMID: 17711589).
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
The results on those studies are not surprising at all.
I've stated that my entire family has had "issues", and just from first hand experience the charts are relate-able for me.
There is something that may not be worked into the data tho. Base line personality.
Coke heads are one type of person, and opiate users are another. So on and so forth.
What the study was comparing were apples, and oranges. Psychedelic users are generally more emotionally balanced (from my opinion but there may be
studies to relate). I don't know IF Psychedelic users are less depressed as a result of the drug(s) or if they were better of in the first place.
The base line depression, and personality issues may have muddied up the results.
I avoid coke heads, can tolerate heroin addicts, take pill freaks for face value (opiates), drunks (no offense Mr Aga) they are fun if I'm drinking
but I'd prefer to be well away from them, trippers on the other hand... I admire many of them. Not so much for the fact that they like Tie Dye, and
cookies but for the fact that simple things make them happy.
As per usual... sweeping generalizations. Yes.
it's not the compounds they choose but instead the underlying personality that leads them to the compounds they choose.
For those of you that understand my "bare bones approach to things, there may be some valuable insights to apply bigger words to in my post.
I would much prefer to see non addictive persons with depression/anxiety whatever studied for comparative results vs. conventional treatment(s).
Including relapse rates, and side effects.
Then the value of addictive "patients" would have more merit. How about DMT to break an LSD addiction? I'd like to see studies on this.
That could fortify many of my personal opinions on the DMT topic. Just because they are both psychedelics does not imply they are the same or even
similar in their course of action.
(you all have already shown this to be correct.
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
That is absolutely worth noting as possible.
There definitely is a proposal out there among some in the medical community that differences in neurology, genetics, or personality can predispose
people to certain drugs (direct or indirectly reinforcing, dopaminergic ones due to predisposition to dopamine depression, for example), but this is
part of why paired samplings in other studies are important and comparison with RCT like I am hoping to see.
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
Exactly! It only took me 15 words.
I get it. People (whether they realize it or no)t will gravitate toward something their body is lacking. Not always but basically.
There are so many complexities in this topic that I never realized. When I simplify the process in my minds eye, I can now understand how frustrating
I can be to those who are aware of the underlying reality in this field of research.
I would have thought,,, Go get a bunch of hobos from the Salvation Army, hook up some wires, feed them sugar cubes, kick back w/ a bottle of Scotch,
and see what happens.
I guess the smart guys rule here. 
[Edited on 4-27-2015 by Zombie]
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
gregxy
Hazard to Others
Posts: 421
Registered: 26-5-2006
Member Is Offline
Mood: No Mood
|
|
| Quote: Originally posted by Chemosynthesis |
That is absolutely worth noting as possible.
There definitely is a proposal out there among some in the medical community that differences in neurology, genetics, or personality can predispose
people to certain drugs (direct or indirectly reinforcing, dopaminergic ones due to .... |
Here is the well know example of Asians and Alcohol which illustrates how genetics can influence response to a drug:
http://en.wikipedia.org/wiki/Alcohol_flush_reaction
I suspect that due to genetics there are subtle differences in the receptors, & enzymes that cause differences in mood and how someone will
respond to a given drug. Someday they will be able to analyze your DNA and figure out exactly what combination of drugs to give you to make you feel
normal (whatever that is).
The other problem is that neurotransmitters and hormones are "time and position dependent signals". The levels change from second to second and they
can have different, even opposing effects in different parts of the brain and body. All that medical science can do now is change the average
levels throughout the body.
[Edited on 27-4-2015 by gregxy]
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
| Quote: Originally posted by gregxy | | I suspect that due to genetics there are subtle differences in the receptors, & enzymes that cause differences in mood and how someone will
respond to a given drug. Someday they will be able to analyze your DNA and figure out exactly what combination of drugs to give you to make you feel
normal (whatever that is). |
While this is true and useful, and is essentially what pharmacogenetics and
pharmacogenomics study to avoid toxicities, this hypothesis I mentioned is more of a basal level dysfunction, where neurotransmitter synthesis or
transport is affected. I think new target identification, dosing and predictions of idiosyncratic immunological responses will be the highlights of
these genomic study techniques. The dopaminergic hypothesis actually is predicated on relatively normal dopaminergic response, rather than
idiosyncratic. A good example is irritable bowel syndrome genome wide association studies. Peripheral serotonin transporter SNPs, which are expressed
in some tissues, seems implicated in serotonergic visceral sensitivity and GI motility... but treatments are generally non-idiosyncratic (though
alosetron has some better results in women). Example treatments are lubipristone or linaclotide for IBS-C subtypes, pregabalin or k-opioids or NSAIDs
for visceral pain. None of these are unique treatments to IBS. SNPs have been correlate with behavior, and the example you give is aversive to alcohol
due to aldehyde buildup, and thus associated with a diminished risk fo alcoholism, for example, but the aldehyde dehydrogenase functions the same way
as a wildtype individual, just with diminished effectiveness. With a SNP in the promoter region, you will influence gene expression (higher/lower) and
with a SNP in the coding region, you will potentially alter the affinity or kinetics of enzymatic reaction, but are unlikely to dramatically affect
signaling. Some other apparent behavioral examplesOI:
10.1371/journal.pone.0099152 and PMID: 25403479. | Quote: | | The other problem is that neurotransmitters and hormones are "time and position dependent signals". The levels change from second to second and they
can have different, even opposing effects in different parts of the brain and body. All that medical science can do now is change the average levels
throughout the body. |
I disagree with this. For one thing, it ignores allosteric drugs, such as is very
common with the GABAa receptor and its multiple drug sites. Also, drug dosing schedules are much more complex than just taking a time resolved average
unless you are maintaining a steady state concentration, as peak concentrations can be very important. Differential compartmentalization also occurs
for various reasons (transport, partitioning, ionization, metabolism), and so average levels throughout the body don't necessarily mean much if
targeting is specific or only paracrine signaling is initiated.
[Edited on 28-4-2015 by Chemosynthesis]
|
|
|
Nicodem
Super Moderator
Posts: 4230
Registered: 28-12-2004
Member Is Offline
Mood: No Mood
|
|
They are surprising for the scientist, as they represent empirical results.
| Quote: | | There is something that may not be worked into the data tho. Base line personality. |
The survey they used as the source of data did not include personality tests, but the authors nevertheless used a multivariate analysis. They looked
for confounding of psychedelic use with the following factors:
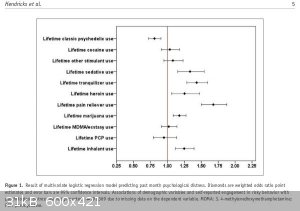
| Quote: | Multivariate logistic regression was used to test the associations between life-
time classic psychedelic use and the primary outcomes while
controlling for the following covariates: age in years (18–25,
26–34, 35–49, 50–64, or 65 or older); gender (male or female);
ethnoracial identity (non-Hispanic White, non-Hispanic African
American, non-Hispanic Native American/Alaska Native, non-
Hispanic Native Hawaiian/Pacific Islander, non-Hispanic Asian,
non-Hispanic more than one race, or Hispanic); educational
attainment (5 th grade or less, 6 th grade, 7 th grade, 8 th grade, 9 th
grade, 10 th grade, 11 th grade, 12 th grade, freshman college year,
sophomore or junior college year, or senior college year or more);
annual household income (less than $20,000, $20,000–$49,999,
$50,000–$74,999, or $75,000 or more); marital status (married,
divorced/separated, widowed, or never married); self-reported
engagement in risky behavior (“How often do you like to test
yourself by doing something a little risky?”; never, seldom,
sometimes, or always) and lifetime illicit use of cocaine, other
stimulants, sedatives, tranquilizers, heroin, pain relievers, mari-
juana, 3,4-methylenedioxymethamphetamine (MDMA)/ecstasy,
phencyclidine (PCP), and inhalants (each aforementioned drug
category coded as separate covariates). All analyses were con-
ducted in SAS version 9.3 using PROC SURVEYLOGISTIC and
accounted for the complex study design variables and sampling
weights as recommended by the NSDUH. |
Some of these factors reflect the demographic and social background of the subjects, which may or may not be connected with personality issues. The
authors do emphasize that the non-availability of some factors may lead to biased results:
| Quote: | Population survey studies cannot control for
all possible sources of confounding and therefore we cannot rule
out that a shared underlying factor may have contributed to both
classic psychedelic use and decreased psychological distress and
suicidality. Psychedelic drug users commonly report autognostic
(Móró et al., 2011), “mind expansion,” spiritual, and curiosity
motives for such use (Lyvers and Meester, 2012). Although these
interests may be lasting effects of classic psychedelic drug use,
they may also represent predrug characteristics among classic
psychedelic users that might protect against suicide as well (e.g.
openness, curiosity, and spiritual tendencies; Carhart-Harris et al.,
2014; Kashdan et al., 2004; Rasic et al., 2009, 2011; Weber and
Pargament, 2014). Lerner and Lyvers (2006) found that classic
psychedelic users reported less materialistic values and greater
mysticism, spirituality, and concern for others than non-classic
psychedelic drug users, and speculated that both predrug factors
and classic psychedelic drug effects contributed to group differ-
ences. This too may be the case with regard to the present find-
ings. However, as classic psychedelic use was associated with
self-reported engagement in risky behavior and illicit substance
use, some who use classic psychedelics may also have a premor-
bid liability for suicidality. The picture is undoubtedly complex.
Nevertheless, future research should attempt to delineate longitu-
dinal predictors of classic psychedelic use that also relate to men-
tal health and suicidal behavior. |
The data from the survey does not support your stereotypes:
| Quote: | Table 1 displays the characteristics of lifetime classic psyche-
delic users versus non-lifetime classic psychedelic users. Lifetime
classic psychedelic use was concentrated among 26–64 year olds
and rare among those aged 65 years and older. Furthermore, life-
time classic psychedelic use was more common among men,
non-Hispanic Whites and Native Americans/Alaska Natives,
those with greater educational attainment and income, individuals
who were divorced/separated or who had never been married,
those with greater self-reported engagement in risky behavior, and
those who reported lifetime illicit use of each of the other sub-
stances. Among lifetime classic psychedelic users, only 240 (0.9%
weighted) reported never having used any other illicit substance
whereas among non-lifetime classic psychedelic users, 85,601
(58.2% weighted) reported never having used any other illicit
drug. |
In fact, the self-reported cocaine use among the "lifetime classic psychedelic drug users" was 71.4%, compared to 7.5% for the "non-lifetime classic
psychedelic drug users" (also, heroin use: 10.6% vs. 0.4%; pain reliever use: 46.5% vs. 9.5%; marijuana: 97.7% vs. 36.2%; and so on). It appears that
the use of psychedelics is way more common among the users of stimulants, opioids, marijuana and other drugs (interestingly, data for alcohol users is
not given!). At least partially, this might have to do with the prohibition laws, skewing the demographics as a factor limiting the use of
psychedelics mostly only to those that are willing to ignore the prohibition as such, rather than reflecting personality connected drug use
preferences. The lower difference in co-use of legal opioids and psychedelics could be an indication of such a prohibition based data distortion
(those willing to use legal opioids, the use of which is still socially barely acceptable, might be more prone to use drugs in general, including
psychedelics - those willing to only use alcohol, tobacco, caffeine and other socially acceptable drugs might be unwilling to use the socially
unacceptable psychedelic drugs).
The prohibition is likely to distort the data in other ways as well, even such that give more credit to your stereotypes. For example, the multi-drug
users are probably much more relaxed in self-reporting psychedelic drug use when compared to prohibition abiding citizens, so perhaps the group of
people whose only drug of choice is a psychedelic may be under represented. If one is willing to report cocaine use, then there is no obstacle in
reporting LSD or mushrooms use as well. On the other hand, if you only use LSD or mushrooms, but no other illegal drug, you might be less willing to
share the information due to the social and legal oppression in a prohibition based society.
| Quote: Originally posted by Zombie | | What the study was comparing were apples, and oranges. Psychedelic users are generally more emotionally balanced (from my opinion but there may be
studies to relate). I don't know IF Psychedelic users are less depressed as a result of the drug(s) or if they were better of in the first place.
|
Like the authors suggested, it is unlikely they were better of in the first place, given that they tend to use a lot of other drugs as well. If they
were better in the first place, it would be unlikely they would be using psychedelic drugs in a country well known for its unusually repressive
attitude toward drug offenders.
| Quote: Originally posted by Zombie | | I avoid coke heads, can tolerate heroin addicts, take pill freaks for face value (opiates), drunks (no offense Mr Aga) they are fun if I'm drinking
but I'd prefer to be well away from them, trippers on the other hand... I admire many of them. Not so much for the fact that they like Tie Dye, and
cookies but for the fact that simple things make them happy. |
From the scientific perspective, your preferences toward disliking/admiring specific drug-type users could be just as much a consequence of your own
personality traits, as is the personality involved in selecting one's drug of choice. You may have confounding factors here.
| Quote: Originally posted by Zombie | | I would much prefer to see non addictive persons with depression/anxiety whatever studied for comparative results vs. conventional treatment(s).
Including relapse rates, and side effects. |
Like it was mentioned several times in this thread, all this has already been done. For example this last article does a good review of the
psychoterapeutic and physiological aspects of psychedelics use:
| Quote: | The past three decades have witnessed a gradual return to
research on classic psychedelics. Though limited in number,
these studies indicate that classic psychedelics may warrant the
attention they received five decades ago, not least in part because
they appear to target a number of factors that modulate suicide
risk. For instance, affective disturbance is one of the most promi-
nent contributors to suicidality (Hawton and van Heeringen,
2009). Under carefully controlled conditions, a single adminis-
tration of psilocybin can occasion profoundly meaningful experi-
ences that bring about persisting elevations in mood among
healthy, hallucinogen-naïve volunteers (Griffiths et al., 2006,
2008, 2011). In a pilot trial among individuals with advanced-
stage cancer a single dose of psilocybin was associated with
long-term reductions in anxiety and depression (Grob et al.,
2011), and in a pilot trial among individuals with life-threatening
diseases two administrations of LSD produced lasting reductions
in anxiety (Gasser et al., 2014; in press). Substance misuse also is
robustly related to suicide risk (Borges et al., 2000; Britton and
Conner, 2010; Center for Substance Abuse Treatment, 2008;
Hawton and van Heeringen, 2009; Wilcox et al., 2004), and sev-
eral lines of research suggest that classic psychedelics have anti-
addictive effects (Bogenschutz and Pommy, 2012). For example,
a recent meta-analysis of six randomized clinical trials of treat-
ment for alcoholism conducted between 1966–1970 found that a
single dose of LSD reduced the probability of alcohol misuse
almost two-fold relative to comparison conditions (Krebs and
Johansen, 2012). Furthermore, a single-arm trial of smoking ces-
sation involving up to three administrations of psilocybin yielded
abstinence rates of 80% at long-term follow-up, more than dou-
bling abstinence rates typical of approved contemporary tobacco
dependence interventions (Johnson et al., 2014). Moreover, natu-
ralistic hallucinogen use predicted a reduced likelihood of recidi-
vism among more than 25,000 individuals under community
corrections supervision with a history of substance involvement
(Hendricks et al., 2014). Additional prominent suicide risk fac-
tors include impulsive-aggressive personality characteristics and
early traumatic life events (Hawton and van Heeringen, 2009).
Psilocybin may occasion enduring improvements in inner peace,
patience, good-natured humor/playfulness, interpersonal regard,
anger, and compassion (Griffiths et al., 2006, 2011), and may
facilitate processing of prior trauma by enhancing recall of auto-
biographical memories (Carhart-Harris et al., 2012a). Finally,
classic psychedelics may boost spirituality (Bogenschutz and
Pommy, 2012; Griffiths et al., 2011), which has been shown to
protect against suicidality (Rasic et al., 2009, 2011; Weber and
Pargament, 2014). Although sample sizes in recent medical
administration studies have been limited, no serious adverse
events were reported, consistent with historical data indicating
that these substances can be administered safely in medical con-
texts by using appropriate safeguards (Johnson et al., 2008).
Neurobiological experiments echo clinical findings, adding
further evidence to suggest that classic psychedelics may modify
processes implicated in suicidality. Increased 5-HT 2A receptor
density in the prefrontal cortex is associated with suicide risk fac-
tors (e.g. major depression) and suicidal behavior, and may
reflect compensatory up-regulation of 5-HT 2A receptors stem-
ming from dysfunctional serotonergic transmission (Bhagwagar
et al., 2006; Carballo et al., 2008; Meyer et al., 2003; Shelton
et al., 2008). Classic psychedelic use down-regulates 5-HT 2A
receptors in the prefrontal cortex which may, in turn, normalize
limbic hyperactivity associated with affective disturbance
(Baumeister et al., 2014, Kraehenmann et al., in press;
Vollenweider and Kometer, 2010). Reduced neuroplasticity (i.e.
expression of brain-derived neurotrophic factor) is also associ-
ated with affective disturbance and suicide, and classic psyche-
delic use may elicit neuroplastic adaptation via glutamatergic
transmission (Baumeister et al., 2014; Bogenschutz and Pommy,
2012; Dwivedi, 2010; Dwivedi et al., 2003; Vollenweider and
Kometer, 2010). Furthermore, the default mode network (DMN)
is hyperactive and hyperconnected among those with affective
disorders, a state that may underpin negative rumination and
rigid pessimism characteristic of these conditions (Carhart-Harris
et al., 2014; Whitfield-Gabrieli and Ford, 2012). Classic psyche-
delics may normalize the DMN, thereby reducing this cognitive
fixedness (Carhart-Harris et al., 2012b; Carhart-Harris et al.,
2014; Muthukumaraswamy et al., 2013; Roseman et al., 2014;
Tagliazucchi et al., 2014). In support of this view, a single dose of
psilocybin increased personality openness 14 months post-
administration (MacLean et al., 2011). Some studies show that
openness may protect against suicide in older adults, though find-
ings are mixed (Segal et al., 2012). Finally, emerging evidence
suggests that classic psychedelics might reduce markers of cen-
tral nervous system inflammation that are implicated in a host of
mental health conditions and suicidal behavior (Black and Miller,
in press; Szabo et al., 2014). |
(I suggest you read the whole article.)
| Quote: Originally posted by Zombie | | Then the value of addictive "patients" would have more merit. How about DMT to break an LSD addiction? I'd like to see studies on this.
|
You can't just make up ideas for trials. Trials are hypothesis based, so you need some understanding of what the treated condition is supposed to be.
For example, there is no such thing as "LSD addiction", so how are you going to find/create your clinical subjects? Psychedelics do not induce craving
and they cause up to one week long tolerance, so that any physiologically based addiction is made impossible. Psychological addiction (if any such
thing even exists) requires regular use and some kind of self-abusive behavior (else it is just a normal compulsion). This is made quite difficult by
the extremely rapid tolerance building and general repulsion from closely repeated use of psychedelics in nearly all people.
But let's assume there was something like an "LSD addiction". DMT could not be used as a replacement drug therapy because it is a full agonist while
LSD is a partial agonist. DMT effects last a few minutes, while LSD lasts for 12 hours. DMT is the only known psychedelic that does not induce
tolerance (probably because its action is too short to cause receptor internalization). So, utmost, LSD could be used as a to treat a hypothetical
"DMT addiction", but not the other way around.
…there is a human touch of the cultist “believer” in every theorist that he must struggle against as being
unworthy of the scientist. Some of the greatest men of science have publicly repudiated a theory which earlier they hotly defended. In this lies their
scientific temper, not in the scientific defense of the theory. - Weston La Barre (Ghost Dance, 1972)
Read the The ScienceMadness Guidelines!
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
My mouse is screwing up, and I can't quote properly. Sorry...
I see problems all over this report, and contradictions galore.
They do agree that demographics are not any sort of bias free basis, and personality testing is not included. In a sense it is because they ASSUME
basic traits, yet they contradict their assumptions.
Example:
" Psychedelic drug users commonly report autognostic
(Móró et al., 2011), “mind expansion,” spiritual, and curiosity
motives for such use (Lyvers and Meester, 2012). Although these
interests may be lasting effects of classic psychedelic drug use,
they may also represent predrug characteristics among classic
psychedelic users that might protect against suicide as well (e.g.
openness, curiosity, and spiritual tendencies; Carhart-Harris et al.,
2014; Kashdan et al., 2004"
next paragraph...
However, as classic psychedelic use was associated with
self-reported engagement in risky behavior and illicit substance
use, some who use classic psychedelics may also have a premor-
bid liability for suicidality. The picture is undoubtedly complex.
Then to finish...
The picture is undoubtedly complex.
Nevertheless, future research should attempt to delineate longitu-
dinal predictors of classic psychedelic use that also relate to men-
tal health and suicidal behavior.
I agree with this.
Not that I could ever claim fame here but a more defined set of parameters has to be established. How much money you pull down is useless data unless
you are comparing rich to poor. Same for most of the "questionnaire" or the ,
Quote:
Multivariate logistic regression system they employed.
Compare addicts blindly. Heroin addicts to cocaine addicts, and both to non addicts.
See who responds to the treatments, and then determine why.
Comparing a heroin addict to a LSD addict is like comparing a drunk to a tree frog.
They are not in the same category.
They are both addictive personalities but for immensely different reasons that WILL skew the results or assumed results.
Quote Zombie:
Coke heads are one type of person, and opiate users are another. So on and so forth.
Quote Nicodem:
The data from the survey does not support your stereotypes:
As I stated above, I believe their data is skewed, and incorrect. They admit so in the first two quotes.
I have a lifetime of experience with many types of addicts, and they are all completely different animals. The only commonality is the predisposition
to addiction, and the inability to solve it themselves.
Ps... I do NOT believe addiction is a disease any more than homosexuality is. Look at how the definitions have changed over the past few decades
alone.
Quote:
Table 1 displays the characteristics of lifetime classic psyche-
delic users versus non-lifetime classic psychedelic users. Lifetime
classic psychedelic use was concentrated among 26–64 year olds
and rare among those aged 65 years and older. Furthermore, life-
time classic psychedelic use was more common among men,
non-Hispanic Whites and Native Americans/Alaska Natives,
those with greater educational attainment and income, individuals
who were divorced/separated or who had never been married,
those with greater self-reported engagement in risky behavior, and
those who reported lifetime illicit use of each of the other sub-
stances
Meaningless to what the mechanism of action is.
Quote:
Among lifetime classic psychedelic users, only 240 (0.9%
weighted) reported never having used any other illicit substance
whereas among non-lifetime classic psychedelic users, 85,601
(58.2% weighted) reported never having used any other illicit
drug.
Backs up my "opinion that they are different from other addicts who will huff gas to get a "high".
Psyc. users are different. Better off mentally IMHO
Edit... I read this wrong. I do not wish to remove my comments here because this finding surprises me. What I would like to see is complete data here.
meaning how much of the other drugs were used.
Did these LSD users spend years shooting dope or did they try it once. Years smoking weed or a few times.
Reporting use, and the amount of use are two completely different factors.
This needs to be more concise to have any relevance.
Quote:
In fact, the self-reported cocaine use among the "lifetime classic psychedelic drug users" was 71.4%, compared to 7.5% for the "non-lifetime classic
psychedelic drug users" (also, heroin use: 10.6% vs. 0.4%; pain reliever use: 46.5% vs. 9.5%; marijuana: 97.7% vs. 36.2%; and so on)
I would like to see these numbers related to the population in general. I imagine the curves would virtually overlap.
I believe they realize this, and backpedal here:
In fact, the self-reported cocaine use among the "lifetime classic psychedelic drug users" was 71.4%, compared to 7.5% for the "non-lifetime classic
psychedelic drug users" (also, heroin use: 10.6% vs. 0.4%; pain reliever use: 46.5% vs. 9.5%; marijuana: 97.7% vs. 36.2%; and so on). It appears that
the use of psychedelics is way more common among the users of stimulants, opioids, marijuana and other drugs (interestingly, data for alcohol users is
not given!). At least partially, this might have to do with the prohibition laws, skewing the demographics as a factor limiting the use of
psychedelics mostly only to those that are willing to ignore the prohibition as such, rather than reflecting personality connected drug use
preferences. The lower difference in co-use of legal opioids and psychedelics could be an indication of such a prohibition based data distortion
(those willing to use legal opioids, the use of which is still socially barely acceptable, might be more prone to use drugs in general, including
psychedelics - those willing to only use alcohol, tobacco, caffeine and other socially acceptable drugs might be unwilling to use the socially
unacceptable psychedelic drugs)
Quote: Originally posted by Zombie
What the study was comparing were apples, and oranges. Psychedelic users are generally more emotionally balanced (from my opinion but there may be
studies to relate). I don't know IF Psychedelic users are less depressed as a result of the drug(s) or if they were better of in the first place.
Like the authors suggested, it is unlikely they were better of in the first place, given that they tend to use a lot of other drugs as well. If they
were better in the first place, it would be unlikely they would be using psychedelic drugs in a country well known for its unusually repressive
attitude toward drug offenders
We are talking about people that don't really care to much for "rules.
Actually I don't recall seeing any AA group for LSD users or support groups advertised on tv like the cocaine, and dope users have.
LSD users are emotionally better off IMHO. I don't need a fella in a white coat that lives in Bele-Aire to guess differently based on his 12 hours of
reading questionnaires to tell me differently. I grew up w/ them. I didn't have to assume anything. My next post here kind of addresses this a bit
more. Sorry if that sounded arrogant.
Quote: Originally posted by Zombie
I avoid coke heads, can tolerate heroin addicts, take pill freaks for face value (opiates), drunks (no offense Mr Aga) they are fun if I'm drinking
but I'd prefer to be well away from them, trippers on the other hand... I admire many of them. Not so much for the fact that they like Tie Dye, and
cookies but for the fact that simple things make them happy.
From the scientific perspective, your preferences toward disliking/admiring specific drug-type users could be just as much a consequence of your own
personality traits, as is the personality involved in selecting one's drug of choice. You may have confounding factors here.
100% agree. It most likely is an opinion based on experience in my life.
I was never robbed by an LSD addict with a gun to my head nor have I ever seen a guy on LSD beating his family with a ball bat because they didn't
have "dope money for them. Violence does not seem to be a part of an LSD users make up.
We all know what other drugs do to addicts. or what other addicts can do. Booze is probably the worst drug when it comes to violent behavior. Booze or
coke... Tough call.
100% agreed... My opinion is most likely bred from my environment(s)
Quote: Originally posted by Zombie
I would much prefer to see non addictive persons with depression/anxiety whatever studied for comparative results vs. conventional treatment(s).
Including relapse rates, and side effects.
Like it was mentioned several times in this thread, all this has already been done. For example this last article does a good review of the
psychoterapeutic and physiological aspects of psychedelics use:
I will read the entire article.
This is where the real effectiveness of treatment can be found.
Comparing different "types of junkies may lead to great discoveries. I am not disputing what MAY come from any sort of research BUT stating you want
to study junkies with Psychedelic drugs just doesn't have the kind of ring to it that would garner much backing.
Stating you want to end depression in elderly, and cancer patients sounds much better.
Let the junkies wait. They are self medicated anyway. Throw them some bongos, a tambourine, and a hand full of joints. They can wait.
Quote:
. For example, there is no such thing as "LSD addiction"
Physically, perhaps not. Mentally? see life long users.
I appreciate your taking the time to discuss this. The whole subject is fascinating, and I believe very valuable.
Perhaps what more of these researchers need is a real interest from the general; public. Like an add company... Tell the world that DMT CAN alleviate
many human conditions, and anyone caught using it without the proper supervision will be thrown in the volcano.
People in general are scared of psychedelics Because of people like Leary, and all those damn hippies that walked around relieving themselves in
yards, parking lots or wherever they happened to be. Free love, and F@ck tomorrow man. Peace!
Psychedelics have a bad reputation. As bad as tobacco IMHO, and it is unjustified. Valium is far worse, and far more deadly but you don't see tie died
Valium shirts.
I respect you immensely Nickodem. You may have no clue how much.
I'm just sharing what I can. My opinion.
[Edited on 5-3-2015 by Zombie]
[Edited on 5-3-2015 by Zombie]
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Nicodem
Super Moderator
Posts: 4230
Registered: 28-12-2004
Member Is Offline
Mood: No Mood
|
|
| Quote: Originally posted by Zombie | I see problems all over this report, and contradictions galore.
They do agree that demographics are not any sort of bias free basis, and personality testing is not included. In a sense it is because they ASSUME
basic traits, yet they contradict their assumptions. |
It is a multivariate analysis, so they did not have much freedom to assume much in the data treatment. In a multivariate analysis you look for
correlations between the factors and the outputs by building a model with as little factor confounding as the data size and distribution allows. They
did some operations in the merging and excluding data, but they described that in the article.
The problems arising from the data and its integrity are survey related and are obvious issues common to every questionnaire based survey (biased
self-reporting, misunderstood questions, errors, etc.). They also expose the problem with the low numerus for certain psychedelic drugs. For example,
for ayahuasca experience the N was only 26 which is 0.008% wighted. DMT was slightly better (N = 391; 0.1%) but still too underrepresented for a
separate evaluation.
| Quote: | I agree with this.
Not that I could ever claim fame here but a more defined set of parameters has to be established. How much money you pull down is useless data unless
you are comparing rich to poor. |
The authors of the study don't have anything to do with personality testing not being included in the National Survey on Drug Use and Health
questionnaire (NSDUH). I assume it is not included because it would double the number of the the already numerous questions. It is a public health
focused survey, so personality is not at its focus. The survey is conducted by a governmental agency: https://nsduhweb.rti.org/respweb/homepage.cfm
| Quote: | | Comparing a heroin addict to a LSD addict is like comparing a drunk to a tree frog. They are not in the same category. |
LSD addicts do not exist, so there is nothing to compare with.
I think time ago there used to be some disorder classification in USA for naming people using psychedelic drugs, but it was most likely removed from
the recent classifications as it made no sense. Even National Institute on Drug Abuse (NIDA), which is a USA governmental agency, does not
recognize any such thing as addiction to psychedelic drugs. It does mention the abuse of psychedelic drugs, but from the context it is obvious they
are actually discussing the normal use of illegal drugs as "abuse" rather than using the term "abuse" for destructive behavior ("a corrupt practice or custom" or "improper or
excessive use or treatment" as per dictionary definitions).
| Quote: |
| Quote: | Table 1 displays the characteristics of lifetime classic psyche-
delic users versus non-lifetime classic psychedelic users. Lifetime
classic psychedelic use was concentrated among 26–64 year olds
and rare among those aged 65 years and older. Furthermore, life-
time classic psychedelic use was more common among men,
non-Hispanic Whites and Native Americans/Alaska Natives,
those with greater educational attainment and income, individuals
who were divorced/separated or who had never been married,
those with greater self-reported engagement in risky behavior, and
those who reported lifetime illicit use of each of the other sub-
stances |
Meaningless to what the mechanism of action is. |
You cannot know which factors are meaningless until you analyze them. Particularly since the mechanism of action for reducing psychological distress
and suicidality is unknown. You are trying to apply non-scientific methods to comprehend a scientific-statistical report. Such approach can only leads
to misinterpretation. In science, a hypothesis comes before the experiment and conclusions come last. Reversing the order leads astray.
| Quote: | Edit... I read this wrong. I do not wish to remove my comments here because this finding surprises me. What I would like to see is complete data here.
meaning how much of the other drugs were used.
Did these LSD users spend years shooting dope or did they try it once. Years smoking weed or a few times.
Reporting use, and the amount of use are two completely different factors.
This needs to be more concise to have any relevance. |
I agree that detailed stories from the users would have greater relevance. Unfortunately, you cannot get such data from a questionnaire-based survey
only. Obtaining such data would require phenomenological methods which have fallen into disdain since researchers, particularly the most incompetent
ones, realized the best way to obtain research grants is by limiting his skills to the scientific method only. Phenomenological studies are also
difficult to publish in journals with an impact factor which is another problem.
Obviously, it is possible and likely that psychedelics are more often used by people addicted to alcohol, sedatives, narcotics or stimulants as some
sort of a self-medication to change their life style. There are plenty of anecdotal reports that this is common practice among alcohol and heroin
addicts. I don't know about stimulant users, but might be similar.
| Quote: |
Quote:
| Quote: | | In fact, the self-reported cocaine use among the "lifetime classic psychedelic drug users" was 71.4%, compared to 7.5% for the "non-lifetime classic
psychedelic drug users" (also, heroin use: 10.6% vs. 0.4%; pain reliever use: 46.5% vs. 9.5%; marijuana: 97.7% vs. 36.2%; and so on)
|
I would like to see these numbers related to the population in general. I imagine the curves would virtually overlap. |
You can easily calculate the numbers for the population in general. The proportion of people who used a psychedelic drug at least once in their life
(coded as "lifetime classic psychedelic drug users") is 13.6% of the population. The proportion of naive people (coded as "non-lifetime classic
psychedelic drug users") is therefore 86.4%. Ponder the data in columns with these coefficients and sum it up to obtain the numbers for the overall
population. The numbers will be somewhat higher than the ones in the "non-lifetime classic psychedelic drug users" column.
| Quote: | We are talking about people that don't really care to much for "rules.
Actually I don't recall seeing any AA group for LSD users or support groups advertised on tv like the cocaine, and dope users have.
LSD users are emotionally better off IMHO. |
Like I already mentioned, I believe it is the reverse. I think the "comorbidity" of LSD use with other drugs usage is probably just because people
using drugs don't care much about rules (prohibition originating bias). Likewise, people in distress are also less likely to care about rules when it
comes to self-medication. This is probably the reason why the study shows that "lifetime classic psychedelic drug users" have so much more troubles
compared to "non-lifetime classic psychedelic drug users". They are demonstrating a survey based statistical fact. They do not make assumptions based
on specific cases.
Besides, how do you make an AA group for LSD users? Maybe: "Hi, my name is John. I spend 12 hours every week tripping on LSD. This does not leave me
enough time to take care of my family and business. I need help." Not really convincing. Even spending 2 hours per day in a traffic jam might a more
convincing issue requiring a AA type support group.
| Quote: | | Stating you want to end depression in elderly, and cancer patients sounds much better. |
You are not being innovative here. Such studies were already conducted and the reports published. However, there is almost nothing on the general
population as an entity. This is why this last study is so valuable.
| Quote: |
Quote:
. For example, there is no such thing as "LSD addiction"
Physically, perhaps not. Mentally? see life long users. |
I'm not sure you know what the term "addiction" means:
http://www.merriam-webster.com/dictionary/addiction
| Quote: | | People in general are scared of psychedelics Because of people like Leary, and all those damn hippies that walked around relieving themselves in
yards, parking lots or wherever they happened to be. Free love, and F@ck tomorrow man. Peace! |
That is not true. In Europe we did not have Timothy Leary and his movement and there was very little propaganda against psychedelics, yet most people
are almost instinctively afraid of them. Some are fascinated, but too afraid to experience. Most chose to remain naive for the rest of their lives. I
believe this is because they sense what a psychedelic experience is, could be, or have their own phantasm about it, and not because they would believe
it is bad for their health, or a danger to the society. You can sense this by seeing how they try to cover the fears with jokes when it comes to the
topic of hallucinogens in general. Rarely they resort to ideological arguments as a defense against the experience. The arguments are more commonly
personal when they decide to share them at all. Maybe it is different in propaganda intensive countries like USA where the survey was conducted, but I
don't know that.
There is another study using the NSDUH data, but from earlier yearly surveys (cited in the here disused article as the only other similar study):
Psychedelics and Mental Health: A Population Study
Teri S. Krebs, Pål-Ørjan Johansen
PLOS, 2013, 8, e63972
DOI: 10.1371/journal.pone.0063972
| Quote: |
Results
21,967 respondents (13.4% weighted) reported lifetime psychedelic use. There were no significant associations between lifetime use of any
psychedelics, lifetime use of specific psychedelics (LSD, psilocybin, mescaline, peyote), or past year use of LSD and increased rate of any of the
mental health outcomes. Rather, in several cases psychedelic use was associated with lower rate of mental health problems.
Conclusion
We did not find use of psychedelics to be an independent risk factor for mental health problems. |
…there is a human touch of the cultist “believer” in every theorist that he must struggle against as being
unworthy of the scientist. Some of the greatest men of science have publicly repudiated a theory which earlier they hotly defended. In this lies their
scientific temper, not in the scientific defense of the theory. - Weston La Barre (Ghost Dance, 1972)
Read the The ScienceMadness Guidelines!
|
|
|
Nicodem
Super Moderator
Posts: 4230
Registered: 28-12-2004
Member Is Offline
Mood: No Mood
|
|
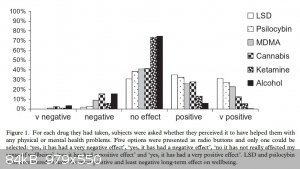
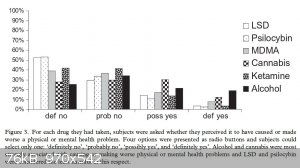
Regarding the survey based studies, there is this interesting web-based questionnaire where psychoactive drug users could report their perceptions on
harm and benefit from their drug use. It kind of complements some of the conclusions made from the NSDUH data analysis. Being volunteered and
web-based it is obviously highly biased in the sense of correspondents selection, but given the questions in the survey and the nature of the study,
this lack is likely not so relevant (it might even be a positive bias, as the correspondents could be more familiar with various drugs and therefore
giving more reliable comparisons).
User perceptions of the benefits and harms of hallucinogenic drug use: A web-based questionnaire study (article here)
R. L. Carhart-Harris, and D. J. Nutt
Journal of Substance Use, 2010, 15, 283-300.
DOI: 10.3109/14659890903271624
One of the authors, Robin Carhart-Harris, has a nice and comprehensive talk on how the psychedelics induce the psychedelic state of mind and how can this be used in psychotherapy. He tries to explain the mechanism of
action on the brain-mind level (the neurochemical aspects were already covered in this thread), all based on his extensive fMRI studies on humans
under the influence of psilocybin (see his publications).
By the way, Zombie, if you want other not too old studies of psychedelics done on "normal subjects", i.e., subjects without particular pathologies, or
not "addicts" as you say, see the study done by Roland R. Griffiths: Psychopharmacology, 187, 268-283 and Psychopharmacology, 218,
649-665 (there is also a TEDx talk where he talks about it). Like I already said, there are several studies like this from the previous century, but some here objected the
old methodologies. Rick Strassman's study on DMT is also similar, but somewhat older.
[Edited on 3/5/2015 by Nicodem]
|
|
|
Fantasma4500
International Hazard
Posts: 1681
Registered: 12-12-2012
Location: Dysrope (aka europe)
Member Is Offline
Mood: dangerously practical
|
|
man this thread is .. long
i 'believe' that there is a positive afterglow with many psychedelics, psilocybin has it and i have even heard 2c-b possess it aswell, up to a whole
week
however for curing depression it almost sounds like just buying whatever nearest dealer can get you would work, i have seen ketamine, 2c-b, weed,
MDMA, LSD and mushrooms suggested for curing depressions. too bad we live in a world where people seem to believe cocaine, heroine and amphetamine is
your friend, and you have a future with it. no arms no cookies, you could say..
when thats said.. i dont think the problem is people being total idiots who cant think a minute into the future, i think the problem lays in the idea
of limiting others.. just this night a bunch of coke addicts messed up my sleep, 3 past midnight, and many people i know do coke and they imagine it
has actual benefits, they see it as a soft drug, for whatever reason, but this doesnt make me want to limit them or the drug either way
think about it.. how many problems arent based on one person trying to or succesfully limiting another?
bigpharma for sure knows the potential of some drugs, and they know those drugs wont get them customers, im as daring as to say that i see a pattern
where bigpharma actually attempts to damage people, so that they can earn further credit by treating them with even more medicine, and then treating
their sideeffects yet again with useless toxic shit
yeah, there is a future in psychedelics, but its a massive taboo, i dont imagine this being done before greed and the like is eliminated, and chances
are everything goes to shit before we reach that point
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
I do tend to generalize, and mis-use words. I know that makes it hard to follow my train of thought.
Quote:
Comparing a heroin addict to a LSD addict is like comparing a drunk to a tree frog. They are not in the same category.
LSD addicts do not exist, so there is nothing to compare with.
I think time ago there used to be some disorder classification in USA for naming people using psychedelic drugs, but it was most likely removed from
the recent classifications as it made no sense. Even National Institute on Drug Abuse (NIDA), which is a USA governmental agency, does not recognize
any such thing as addiction to psychedelic drugs. It does mention the abuse of psychedelic drugs, but from the context it is obvious they are actually
discussing the normal use of illegal drugs as "abuse" rather than using the term "abuse" for destructive behavior ("a corrupt practice or custom" or
"improper or excessive use or treatment" as per dictionary definitions).
I use the word addict quite liberally. It's like saying someone is addicted to kittens.
In all fairness I don't really see any difference. If you are physically addicted to something or mentally addicted you still have an issue.
That interconnects to the "does DMT physically change you or does it mentally change you.
Interesting question, and the answer is important (at some point) but if DMT can break either "type" of addiction, then the words I use are less
important. It become a potato / potaato conversation.
I get the fact that for science all the words have to be exact. Just as in law because after all the two are bed partners, like it or not.
Quote Nickodem:
You can easily calculate the numbers for the population in general. The proportion of people who used a psychedelic drug at least once in their life
(coded as "lifetime classic psychedelic drug users") is 13.6% of the population. The proportion of naive people (coded as "non-lifetime classic
psychedelic drug users") is therefore 86.4%. Ponder the data in columns with these coefficients and sum it up to obtain the numbers for the overall
population. The numbers will be somewhat higher than the ones in the "non-lifetime classic psychedelic drug users" column.
Did I read this correctly?
"The proportion of people who used a psychedelic drug at least once in their life (coded as "lifetime classic psychedelic drug users") is 13.6% of the
population"
Use LSD once, and it is coded as Lifetime user? Then I must be a lifetime soccer player.
That makes no sense to me.
Quote:
We are talking about people that don't really care to much for "rules.
Actually I don't recall seeing any AA group for LSD users or support groups advertised on tv like the cocaine, and dope users have.
LSD users are emotionally better off IMHO.
Like I already mentioned, I believe it is the reverse. I think the "comorbidity" of LSD use with other drugs usage is probably just because people
using drugs don't care much about rules (prohibition originating bias). Likewise, people in distress are also less likely to care about rules when it
comes to self-medication. This is probably the reason why the study shows that "lifetime classic psychedelic drug users" have so much more troubles
compared to "non-lifetime classic psychedelic drug users". They are demonstrating a survey based statistical fact. They do not make assumptions based
on specific cases.
I really need to know the definitions here. Lifetime vs. non Lifetime.
Obviously a person that uses all sorts of drugs will have more issues as compared to a dedicated LSD user or any other single drug user for that
matter.
I'm basing this on "functional" users. Those that keep a job, ect... vs the laying in the street user.
Quote Nickodem;
"Besides, how do you make an AA group for LSD users? Maybe: "Hi, my name is John. I spend 12 hours every week tripping on LSD. This does not leave me
enough time to take care of my family and business. I need help." Not really convincing. Even spending 2 hours per day in a traffic jam might a more
convincing issue requiring a AA type support group.
Lol... Hi I'm Ken, and I forgot why I'm here. You gonna eat those cookies?
I beats the crap out of ...
Yo! I'm Pete. I beat my kids, and drink 1 fifth of vodka for breakfast. I don't have a problem but the court sent me here. Anyone have a F'n problem
with that?
LSD AA groups would be too much fun. In fact I think I do know of one. It's on PBS every week. The McLaughlin Group.
Quote:
Stating you want to end depression in elderly, and cancer patients sounds much better.
You are not being innovative here. Such studies were already conducted and the reports published. However, there is almost nothing on the general
population as an entity. This is why this last study is so valuable.
You know what?
Focus on one group. Keep making them better. They don't even apply what they know works!
Why keep this "shotgun" style research going if they do not apply it where it is KNOWN to work?
Once Bob, and Ginny start talking about how much better their family life is due to Grandma taking DMT, and how much more comfortable Susan is with
Chemo since the DMT treatments... It might get a foothold, and be considered a valuable tool.
Like I said... Let the junkies rot for a minute. They're not going anywhere.
Fix the contributing members of society first. Prove the research is correct, and the treatment is viable instead of studying everything else for a
minute.
It's just wasting time, and allowing the hurt to continue.
They find that something does not work somewhere, and it's ammo in the chamber for the nay sayers.
Quote:
People in general are scared of psychedelics Because of people like Leary, and all those damn hippies that walked around relieving themselves in
yards, parking lots or wherever they happened to be. Free love, and F@ck tomorrow man. Peace!
That is not true. In Europe we did not have Timothy Leary and his movement and there was very little propaganda against psychedelics, yet most people
are almost instinctively afraid of them.
That's solely due to what happened here in the US. European kids fell into that hippy shit because it was a fad.
You didn't need Leary there. He did enough damage for the entire planet to share.
Granted he was correct on MANY levels. He was just overly zealous. The harm was done in the '60s, and the repercussions are still with us. IMHO.
Quote:
Results
21,967 respondents (13.4% weighted) reported lifetime psychedelic use. There were no significant associations between lifetime use of any
psychedelics, lifetime use of specific psychedelics (LSD, psilocybin, mescaline, peyote), or past year use of LSD and increased rate of any of the
mental health outcomes. Rather, in several cases psychedelic use was associated with lower rate of mental health problems.
Conclusion
We did not find use of psychedelics to be an independent risk factor for mental health problems.
We all agree on this. It's obvious.
It's the arguements against that are the "wall" that must be removed.
Another point that we are wandering away from is DMT is really what I believe is sort of the "wonder drug" here.
The others like LSD, Peyote, ect, are all similar but not the same.
DMT research is what I would like to know more about.
Thanks Nickodem for putting up w/ my lack of complex sentences, and simplistic manor. I believe you do understand we are on the same side in these
matters.
Edit;
Thanks. I'm looking this up... Roland R. Griffiths: Psychopharmacology, 187, 268-283 and Psychopharmacology, 218, 649-665 (there is also a TEDx talk
where he talks about it)
It's so hard to find all the time needed.
[Edited on 5-3-2015 by Zombie]
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
| Quote: Originally posted by Antiswat | man this thread is .. long
i 'believe' that there is a positive afterglow with many psychedelics, psilocybin has it and i have even heard 2c-b possess it aswell, up to a whole
week
however for curing depression it almost sounds like just buying whatever nearest dealer can get you would work, i have seen ketamine, 2c-b, weed,
MDMA, LSD and mushrooms suggested for curing depressions. too bad we live in a world where people seem to believe cocaine, heroine and amphetamine is
your friend, and you have a future with it. no arms no cookies, you could say..
when thats said.. i dont think the problem is people being total idiots who cant think a minute into the future, i think the problem lays in the idea
of limiting others.. just this night a bunch of coke addicts messed up my sleep, 3 past midnight, and many people i know do coke and they imagine it
has actual benefits, they see it as a soft drug, for whatever reason, but this doesnt make me want to limit them or the drug either way
think about it.. how many problems arent based on one person trying to or succesfully limiting another?
bigpharma for sure knows the potential of some drugs, and they know those drugs wont get them customers, im as daring as to say that i see a pattern
where bigpharma actually attempts to damage people, so that they can earn further credit by treating them with even more medicine, and then treating
their sideeffects yet again with useless toxic shit
yeah, there is a future in psychedelics, but its a massive taboo, i dont imagine this being done before greed and the like is eliminated, and chances
are everything goes to shit before we reach that point |
In the simplest f terms I agree with most all of what you say here.
In the '80s, coke ruled the day. It was then, and probably still is considered "soft" by most users.
Chemosynthises pointed out the Big Pharma problems, and yes, I fear you may be right... There may well be no more "Us" before they figure "Us" out.
Sometimes all of this discussing seems pointless but it beats sitting in the local bar talking about what car is faster, and why.
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
The idea that competing pharmaceutical companies somehow collude to poison humanity on a mass scale with unparalleled precision rather than get
exposed by competitors, academics, and regulators (any of whom would make their careers, land movie deals Erin Brokovitch style, and score talk
circuit retirement laps over that alone), is not only detached from the reality of how drug discovery and design works (in public or private
industry), but a gigantic risk of jail time and nonsensical in light of increased drug development costs.
Why diminish your profit margins on a short term gain, risk ruining your company and prison if just one person in a government, academia, another
company, or your own company (formerly or current) decides to go public? It's not like disease itself is going away. Plenty of diseases out there
people would pay just as much to treat or more to eradicate. You basically have to indict every single scientist in any biologically oriented field,
and much of chemistry, to believe this, as well as assume they have no conscious or loved ones with an illness they would personally like to see
treated or cured, then largely ignore how pharmaceutical medicine has advanced at some arbitrary point of conspiracy.
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
Side effects. Ever see all those late night lawyers?
How about the newest must have allergy pill?
When they list Rectal bleeding , flu, , cancer, enlarged breasts as potential side effects just to help you stop sneezing... I get where Antiswat was
coming from.
Like me... He could have worded that better but I get the idea.
Here 26 side effects that come with many prescription drugs currently on the market.
Drainage, crusting, or oozing of your eyes or eyelids
Swollen, black, or "hairy" tongue
Changes in the shape or location of body fat
Decrease in testicle size
Sores or swelling in your rectal or genital area
Blue lips or fingernails
Purple spots on your skin
White patches or sores inside your mouth or on your lips
Irregular back-and- forth movements of your eyes
Enlarged breasts in males.
Unusual risk-taking behavior, no fear of danger
Extreme fear
Hallucinations, fainting, coma
Fussiness, irritability, crying for an hour or longer
Paralysis
Thoracic Hematoma (bleeding into your chest)
A blood clot in your lung
Liver damage
Kidney damage
A lump in your breast
Decreased bone marrow function
Congestive heart failure
Shingles
Nerve pain lasting for several weeks or months
Bleeding that will not stop
Coughing up blood or vomit that looks like coffee grounds
One drug on the market, EvaMist -- a treatment for menopause symptoms such as hot flashes -- has possible side effects that include cancer, stroke,
heart attack, blood clots, and dementia!
But this is only a partial list of the potential side effects of prescription drugs. There are, unfortunately, many more out there.
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
You are seriously going to ask if I'm familiar with side effects of drugs? Do you know that drug companies often have to list suspected side effects
with tenuous associations to drugs due to how clinical trial and side effect reporting is handled? Who bothers reading those information sheets
anyway? Patient compliance, much less reading the booklet, is hard enough.
When someone says "i see a pattern where bigpharma actually attempts to damage people, so that they can earn further credit by treating them with
even more medicine, and then treating their sideeffects yet again with useless toxic shit" they are insinuating that drug companies are purposefully
designing flaws, presumably type A adverse effects, into drugs with such skill and precision to allow easy remediation, while still getting past
approval and avoiding enough negative publicity to kill a company... and that on top of that, everyone is too stupid to catch on, much less a
competitor? That is so patently ridiculous it's unbelievable, and that's being generous on my interpretation of the quote; they really said that
companies are releasing drugs with zero efficacy, yet demonstrated toxicity at purportedly therapeutic doses. There is absolutely no evidence for this
whatsoever.
Drug companies are competing with one another. Releasing a drug that purposefully has a higher incidence of expected side effects for actuarial
purposes is one of the most mentally handicapped things a drug company could do! All a competitor has to do is float that hypothesis to the
anti-vaccine Scientologist types, or a hungry reporter looking to break a huge story, and they gain conceded market sure. That also gives way too much
credit to the omnipotence of pharmacological science. We can't even predict type B adverse effects well enough, as late stage liver problems are the
largest reason for drug failures after spending fortunes on pre-clinical and early clinical testing. You would think a drug company would stop
throwing money away before investing in a hair-brained scheme to physiologically hurt the public, possibly even themselves. No one with a clue would
honestly believe that a company were capable of, much less willing to invest time, money and effort into, such a gambit. It's an incredible insult to
anyone working in a pharmaceutical company, biotech, a regulatory agency, academic institution, or hospital involved in any aspect of research to
suggest they are either morally bankrupt and complicit or stupid enough to be involved in that.
You don't see physicians or nurses poisoning patients just to sell them more services, do you? Sometimes you get a quack who kills patients, but that
can be counterproductive to the whole make money spiel. What makes it so much more likely that a big evil, impersonal company bogeyman manages it on a
mass scale without anyone noticing, yet there is no evidence of this? There can't be enough money in one company to buy off every government scientist
at every level of government regulation, assuming all were evil. If there were, wouldn't it be cheaper to malign competition? What about the
perpetrators who would presumably want safe drugs? Do you set up some kind of secret secondary synthesis and research apparatus? What about
distribution? Suddenly you need what amounts to double the effort of just making a functional drug. Designing drugs with fewer adverse side effects
would be a better sell because it could likely be taken by more people more frequently with easy marketing as super safe and patient friendly, and
make a ton of money. Then you could push it on patients who are hypochondriacs, or think an antibiotic would help with their cold, etc.
[Edited on 4-5-2015 by Chemosynthesis]
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
I wasn;t questioning you or what you know. It was a statement question.
Of course we all understand your point on this.
I'm just saying, I'd rather put up with watery eyes, than rectal bleeding.
if I meet a gal, and she tells me there is a one in one hundred chance I will bleed out my butt if I sleep w/ her... I'm going home alone.
Yeah poison drugs to sell you more drugs to take care of the poison is ridiculous... So is a bleeding but for hay fever treatment. That's all I'm
agreeing with.
(i should have picked a better example)
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
gregxy
Hazard to Others
Posts: 421
Registered: 26-5-2006
Member Is Offline
Mood: No Mood
|
|
Well one of those NSAIDs DID make me bleed out of my butt. Fortunately I had read the warnings knew to stop taking it.
I don't believe drug companies would market something harmful but the WILL pass up the best treatment simply because its not profitable.
Here is a case in point. Clomid, has been around so long it has lost patent protection. It is the best choice for treating low testosterone levels
in men.
Yet no drug company will offer it since there is no way to make money on it.
http://shiramillermd.com/blog/clomid-men-testosterone-altern...
http://www.prohormonepodcast.com/prohormones/enclomiphene-ci...
|
|
|
Zombie
Forum Hillbilly
Posts: 1700
Registered: 13-1-2015
Location: Florida PanHandle
Member Is Offline
Mood: I just don't know...
|
|
LOL... I bookmarked the links.
They tried to have me "put to sleep" so I came back to return the favor.
Zom.
|
|
|
Chemosynthesis
International Hazard
Posts: 1071
Registered: 26-9-2013
Member Is Offline
Mood: No Mood
|
|
Any NSAID with COX affinity can give a GI bleed or ulceration, which could could present in either fecal or vomit blood. The more selective ones are
better are not causing this.
Enclomifene is actually in clinical trials for testosterone replacement therapy in men, and can always be written off-label at the whim of a
physician. See clinical trial NCT01270841.
|
|
|
| Pages:
1
..
4
5
6
7
8 |
|